
Hongyan Liu *, MD, Laichun Song *, MD, Ming Qi, MD, Bihui He *, MD
Division of Cardiac Surgery, Wuhan Asia Heart Hospital, Wuhan University of Science and Technology, Wuhan, China
*Corresponding author: Bihui He, MD, No.753 Jinghan Road, Hankou District, Wuhan, P.R. China.
Received Date: September 01, 2023
Accepted Date: October 08, 2023
Published Date: November 20, 2023
Citation: Liu H, Song L, MD, Qi M, MD, He B. (2023) “A Novel Endovascular Method to Treat a Post-Arch-Repair Chronic Aortic Dissection Aneurysm.” J Clinical Cardiology Interventions, 3(2); DOI: http;//doi.org/10.2023/07.1038.
Copyright: © 2023 Bihui He. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The technique was demonstrated in a 60-year-old man with a history of type A aortic dissection, who was referred for the Sun’s procedure in 2016. Follow-up computed tomography (CT) showed a chronic thoracic false lumen aneurysm of 8.8 cm, and the patient underwent endovascular treatment with covered stent grafts combined with a hand-crafted candy-plug device to rule out chronic aortic dissecting aneurysm (CADA) and preserve lower body perfusion. Post-operative recovery was uneventful. CT showed a completely thrombosed thoracic CADA with no endoleak. The combination of covered stent grafts and the candy-plug device could be used to treat CADA and preserve these false lumen perfused vessels, especially when existing frozen elephant trunk(FET) stents are present in a suitable landing zone.
Introduction
Frozen elephant trunk (FET) technology for aortic dissection repair was introduced more than two decades ago. However, the complications of FET, including a residual false lumen can develop into dissection aneurysms and these enlarged false lumen are often located in the visceral segment of the descending thoracic aorta. We present a case of chronic post aortic dissection aneurysm (CADA) after arch replacement and a new endovascular treatment options to address these issues.
Endovascular ProcedureA 60-year-old man was diagnosed with type A aortic dissection and underwent the Sun’s procedure six years ago.The most recent follow-up CT showed the entire descending thoracic aorta was significantly dilated to an 8.8 cm aneurysm(Fig. 1).
 Figure 1: Prior FET stented intimal flap and large thoracic CADA.
Figure 1: Prior FET stented intimal flap and large thoracic CADA.
Symptoms of upper back pain had appeared in the last 2 months. Both the symptoms and the size indicated the need for intervention. Patients were admitted to the catheterisation laboratory under general anaesthesia. Two guidewires (Cook Group, Lunderquist, Bloomington, IN, USA) were passed through the true and false lumen from the bilateral femoral sheaths. A commercially available bifurcated body stent graft had been used for abdominal endovascular aortic repair (32120 mm Lifetech, AnkuraAAA, Shenzhen, China) was delivered through the true lumen and deployed 5 mm from the top of the existing FET holder. The two limb lengthening grafts (14120 mm Lifetech, Shenzhen, AnkuraAAA) were attached to the bifurcated body stent to form the true and false lumen. To completely block retrograde blood flow in the enlarged false lumen, a 120mm long, 37mm diameter stent (WL Gore and Associates, TAG, Flagstaff, AZ, USA) was modified by adding a diameter-restricting suture in the centre of the stent prior to deployment (Fig. 2).
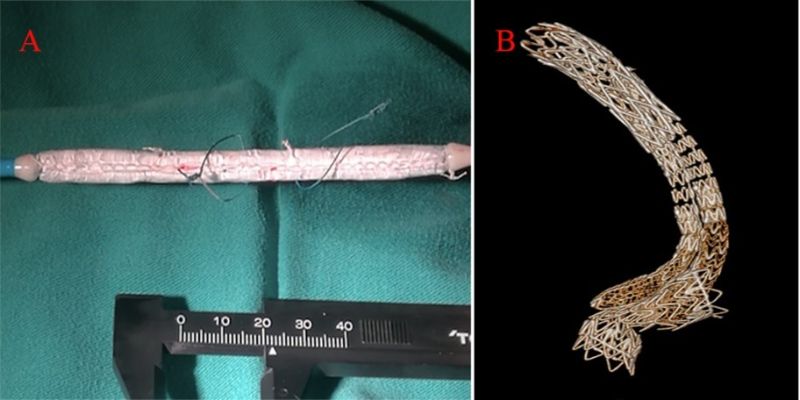 Figure 2: (A) Handmade 37 100 mm candy plug device. (B) The endograft structure after deployment.
Figure 2: (A) Handmade 37 100 mm candy plug device. (B) The endograft structure after deployment.
This customisation was shaped like a wrapped candy with a waist of only 14 mm in diameter. The central tunnel size of the candy plug device was determined by the length of the two Tycron threads. The device is deployed in the narrowest false lumen segment of the diaphragm. An additional limb-extending stent graft (16120-mm WL Gore and Associates, Excluder, Flagstaff, AZ, USA) was delivered and deployed for a false intraluminal graft attached to the candy plug central tunnel. Completion angiography showed no residual flow into the false lumen aneurysm. Post-operative recovery was uneventful. Follow-up CTA at 1 month showed a thoracic false lumen aneurysm thrombus without endoleak. (Fig. 3).
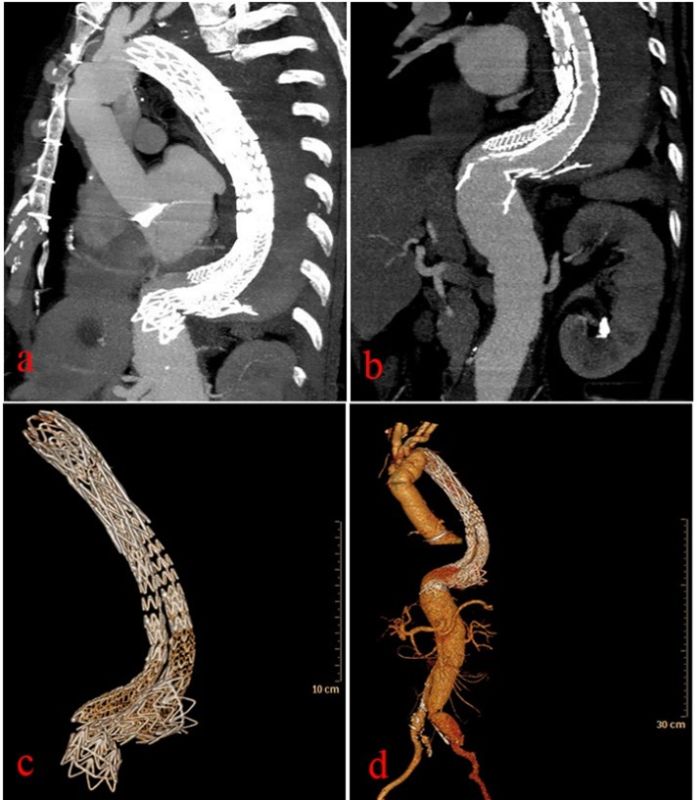 Figure 3: CADA reduced on postoperative CT scan.
Figure 3: CADA reduced on postoperative CT scan.
Discussion
The widespread use of FET stenting is associated with the development of post-dissection aneurysms (1), which present additional technical challenges. The visceral branches originate from the false lumen usually makes overall planning difficult. Fenestrated and branched TEVAR (F/Br-TEVAR) was shown to be a feasible treatment for chronic post-dissection aneurysms (2). However, this technique has been limited to a few centres of expertise. The candy-plug technique for distal exclusion of a false lumen was described by Kölbel et al (3) and Ogawa introduced its use in the Gore Excluder Extender (4). We use the candy-plug device not only as a vessel plug, but also as a calibre-limiting tool that forms a central tunnel. A hand-crafted candy plug provides a tool to exclude the neck of larger aneurysms and provides central access to the blood supply.Our new approach can also be considered as a functional fenestration of lower body perfusion, where in addition to distal exclusion of CADA, blood flow is directed to aortic branches dependent on the false lumen and limited by the central tunnel calibre. Although the initial post-operative images met our expectations - anurysm sac thrombosis, no endoleak and good lower body perfusion. However, the size of the true and false lumens must be closely monitored.
Conclusion
The combination of covered stent graft and a candy plug device can treat CADA and preserve these false lumen perfused vessels, especially when existing FET stents are present in a suitable landing zone.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org